Recently, I had the privilege of attending a lecture by Dr. Katia López, a board member of the Santa Cruz Surgical Society, during the 2026 International Multidisciplinary Medical Congress. The central theme was a necessary reality check: “Robotic Surgery: The Present and the Future.”
Many of us students wonder: why does robotics still feel like a distant dream in our region while countries like Brazil have been accumulating decades of experience? Dr. López not only answered this question but guided us through a technical journey, demystifying what it actually means to operate with a robot.
The “surgeon’s ladder”: natural evolution
One of the most compelling points of the lecture was the analogy of the “Surgeon’s Ladder.” You cannot reach robotics without traveling the fundamental path first. According to the speaker, robotic surgery is not an isolated revolution, but the natural evolution of advanced laparoscopy.
Modern surgical training requires structured progress:
- Open Surgery: The foundation of everything.
- Basic Laparoscopy: Mastering triangulation (e.g., appendectomies and cholecystectomies).
- Advanced Laparoscopy: The bariatric or complex hernia surgeon.
- Robotic Surgery: The pinnacle of precision and ergonomics.
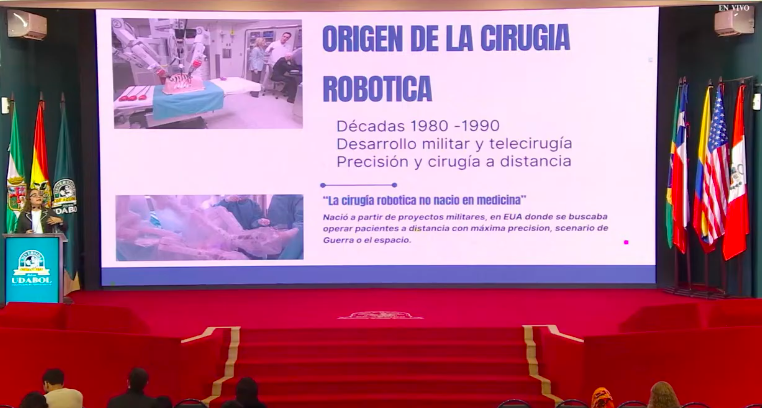
What is robotic surgery, really?
We must discard the idea that the robot operates on its own. The Da Vinci platform (born from military tele-surgery projects in the 1980s and 90s) is actually a high-precision interface. The surgeon sits at a console, controlling robotic arms with millimetric movements that eliminate human physiological tremor.
The pillars of the system:
Surgeon’s Console: Where the doctor commands everything with 3D vision and absolute precision.
Patient Cart: Where the arms holding the instruments are located.
Vision Tower: The visual “brain” that processes the images.
The surgical “corset”: clinical case of hernia and diastasis
Dr. López demonstrated a case of rectus diastasis and umbilical hernia resolved via robotics. The key concept here was the use of CO2 as a dissector. By insufflating the cavity, the gas assists in the automatic separation of tissues, facilitating the creation of flaps.
The closing of the hernia defect was described as crafting a “corset”—an inverted suture with polydioxanone (PDS) thread that safely approximates the tissues. Direct visualization allowed for a precision in mesh placement that would be far more laborious in conventional laparoscopy.
Why don’t we have robots everywhere?
The speaker was honest about the bottlenecks in Bolivia and much of Latin America:
Capital Cost: $2.5 million just for the equipment.
Infrastructure: It is not enough to buy a robot; a hybrid hospital is needed, integrating tomography, MRI, and endoscopy.
Maintenance: The need for specialized biomedical engineering for complex repairs.
Accessibility: The cost per procedure remains prohibitive for universal public systems.
Conclusion: the role of the medical student
The final message is inspiring: we cannot close our eyes to the future. Robotics will arrive, and we will be the surgeons operating them. The key is not the rush to own the machine, but the perfection of laparoscopic technique.
As Dr. Katia aptly stated, robotics began as a necessity to operate with precision where the surgeon could not be present. Today, it is the state of the art. Study hard, practice triangulation, master laparoscopy, and be prepared: the future of surgery is technological, but the hand that commands it must still be human and excellently trained.
Did you like this summary? Don’t forget to comment and share it with your medical school colleagues!
About Educar Med
Educar Med isn’t just about passing tests; it’s about rejecting clinical mediocrity. We are a community dedicated to training the new generation of physicians who think, examine with precision, and transform lives.
Keep raising your clinical standards. Follow Educar Med on social media: