I recently had the opportunity to follow the brilliant lecture delivered by Dr. Sergio León, a general surgeon trained at the Universidad del Valle (Cali, Colombia), during the 2026 International Multidisciplinary Medical Congress. Under the title “Traspasando fronteras anatómicas: el presente y el futuro de la cirugía mínimamente invasiva” (Beyond Anatomical Borders: The Present and Future of Minimally Invasive Surgery), the speaker provided a highly practical approach tailored for medical students. He demystified the roles of laparoscopy and video-assisted thoracoscopic surgery (VATS) in both elective settings and the high-stakes environment of emergency trauma. Below, I share my critical analysis and the primary clinical insights we must master to move far beyond surgical rote memorization.
The core theme of the presentation centers on a paradigm shift in how we approach the body’s internal cavities. Dr. León argues that minimally invasive surgery (MIS) is no longer a distant future but the absolute present of medicine. However, he also delivers a reality check for our region: while robotics and digital platforms dominate cutting-edge centers, the true frontier of MIS in Latin America remains accessibility. Many community and rural hospitals still lack basic laparoscopy towers, forcing surgeons to master traditional open techniques with equal proficiency.
Key concepts and the physiology behind MIS
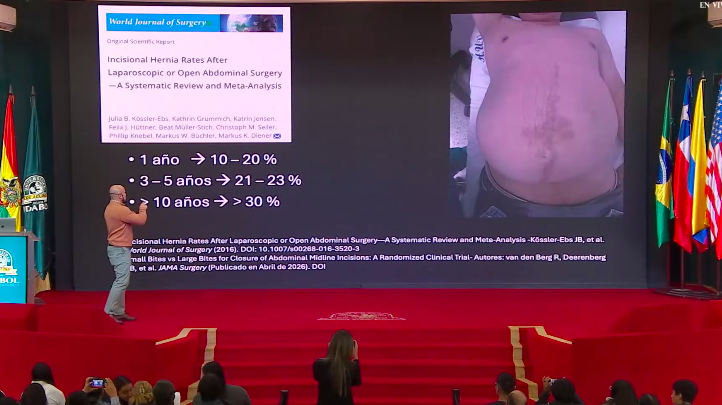
The first point that stood out to me in the lecture was the deconstruction of the “metabolic cost” of a large surgical incision. Opting for an open laparotomy or thoracotomy is never a benign choice; it imposes severe trauma on the abdominal wall and triggers a much greater systemic inflammatory response. To illustrate this, the speaker presented striking statistical data regarding the cumulative risk of developing incisional hernias over time in patients subjected to open surgeries:
- At the 1-year mark post-op: 10% to 20% risk of herniation.
- Between 3 and 5 years post-op: 21% to 23% risk.
- Beyond 10 years post-op: The risk surpasses the 30% mark.
Conversely, the logic of MIS is anchored in anatomical preservation. Modern high-definition optics provide the surgeon with a magnified field, enlarging internal structures on the monitor up to 10 times compared to the naked eye.
Operationally, we must clearly differentiate the physical dynamics of the two primary cavities involved:
Laparoscopy: Targeted at the peritoneal cavity, it requires the creation of a pneumoperitoneum via the controlled insufflation of carbon dioxide ($CO_2$), necessitating multiple entry ports (trocars).
Video-Assisted Thoracoscopic Surgery (VATS): Performs within the pleural cavity. Here, the physical dynamics shift entirely: little to no $CO_2$ is used. Instead, the working space is generated by inducing a selective lung collapse on the operated side. Another massive advantage is that VATS is far more conservative with access points, frequently requiring only 1 or 2 intercostal ports.
Macroscopic findings and key signs (visual semiology)
One of the highlights of the lecture was the practical demonstration of real clinical cases through diagnostic laparoscopy videos. Dr. León reinforced how direct visualization in MIS serves as a powerful diagnostic tool when conventional imaging leaves a clinical blind spot. Three classic pathognomonic visual findings were showcased, serving as excellent diagnostic anchors for us:
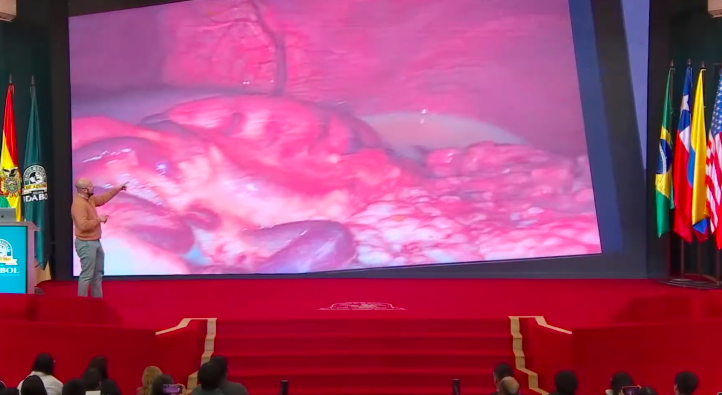
1. Steatonecrosis in acute pancreatitis
When analyzing a case of refractory acute abdomen, the surgeon demonstrated the presence of multiple firm, yellowish-white plaques scattered across the peripancreatic adipose tissue and mesentery. This is steatonecrosis (often described as “candle-dripping” or fat necrosis), generated by the enzymatic digestion of fat from extravasated pancreatic enzymes. Keep this fundamental clinical reminder in mind: acute pancreatitis is eminently a medically managed condition, and evaluating the cavity via laparoscopy occurs primarily to resolve diagnostic uncertainty in emergencies.
2. Peritoneal and pleural tuberculosis as “grains of rice”
A chronic ascites case undergoing investigation revealed a peritoneal cavity (and later, a pleural cavity in a different patient) completely carpeted by tiny, millimeter-sized whitish nodules. Visually identical to peritoneal carcinomatosis (malignant tumor dissemination), this “grains of rice” appearance is the classic macroscopic signature of extrapulmonary Tuberculosis. Laparoscopy in these scenarios is mandatory to safely obtain a direct excisional biopsy.

3. Chylous ascites resembling “condensed milk”
The speaker demonstrated an advanced case of gastric cancer (Stage IV) where tumor cells invaded and obstructed the main lymphatic drainage pathways. The visible result during laparoscopy was the accumulation of chyle within the cavity, generating a thick, opaque, purely milky ascites fluid with the distinctive macroscopic appearance of “condensed milk.”
Additionally, regarding elective and general emergency surgery, it was reinforced that adhesions (fibrous bands) remain the leading cause of mechanical small bowel obstruction worldwide, followed closely by abdominal wall hernias.
Clinical applications, trauma algorithms, and decision-making
The lecture successfully shattered the myth that politraumatized patients cannot benefit from minimally invasive approaches. They certainly can, provided the Golden Rule of Trauma is strictly respected: the patient must display persistent hemodynamic stability (Systolic Blood Pressure greater than 90 mmHg). If shock or refractory hypotension is present, MIS is absolutely contraindicated, requiring immediate open laparotomy or thoracotomy.
In the realm of surgical tactics and decision-making, the following practical scenarios were reviewed:
- Left Thoracoabdominal Wounds: This is a crucial anatomical rule. Every stable patient with a penetrating wound (stab or gunshot) in the left thoracoabdominal transition zone must undergo surgical evaluation (laparoscopy or VATS) to inspect the diaphragm. Due to the pressure gradient (negative pressure in the thorax and positive pressure in the abdomen), small, occult lacerations in the left diaphragm will inevitably progress into delayed diaphragmatic hernias, causing the stomach, colon, or spleen to translocate into the chest. On the right side, the liver acts as a massive anatomical barrier, removing this systematic obligation.
- Absolute Conversion Criteria: During a trauma laparoscopy, if the surgeon encounters an expanding or pulsatile retroperitoneal hematoma, the procedure must be converted to an open laparotomy immediately. This finding indicates a major retroperitoneal vascular injury (such as the abdominal aorta or vena cava), which cannot be safely managed given the space and time constraints of MIS.
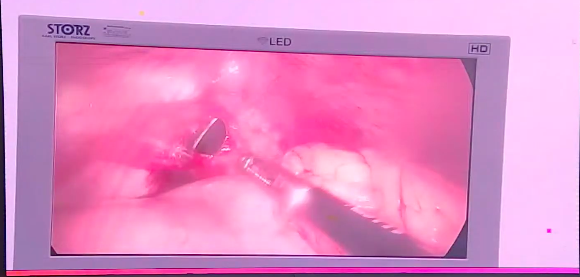
- Conservative Management via Pericardial Window: One of the most impressive video cases showed a stable patient with a precordial stab wound. Utilizing VATS, the surgical team performed a pericardial window. After aspirating the hemopericardium and irrigating the cavity, they confirmed that the myocardial injury had already self-tamponaded spontaneously and was not actively bleeding. In a high-volume, experienced trauma center, the decision was made to manage the patient conservatively, sparing the youth an aggressive sternotomy.
I conclude my analysis by highlighting Dr. León’s final message on medical training. Developing proficiency in MIS, such as performing intricate intracorporeal suturing with laparoscopic needle drivers, demands a steep learning curve and exhaustive simulation using pelvic trainers or dedicated software. As medical students, we must pursue this practical excellence early; a refined anatomical understanding paired with technical precision is what ultimately dictates true surgical success.
About Educar Med
Educar Med isn’t just about passing tests; it’s about rejecting clinical mediocrity. We are a community dedicated to training the new generation of physicians who think, examine with precision, and transform lives.
Keep raising your clinical standards. Follow Educar Med on social media: