As we transition from basic sciences to clinical rotations and on-call shifts, a superficial understanding of anatomical and physiological concepts becomes insufficient. The distinction between an artery and a vein, often treated as rudimentary, is a classic example. In medical practice, neglecting these details can compromise everything from a simple venipuncture to the invasive monitoring of a critical patient.
This article is designed to consolidate your knowledge. We will dissect the histological, hemodynamic, and clinical differences between resistance vessels and capacitance vessels, using clinical reasoning as our guide.
Definitions and direction of blood flow
The fundamental criterion for differentiating arteries from veins is not the oxygen content of the blood they carry, but rather the direction of flow relative to the heart:
- Arteries: These are efferent vessels, meaning they carry blood away from the heart to the peripheral tissues (with the notable exception of the pulmonary artery).
- Veins: These are afferent vessels, carrying blood from the peripheral tissues back to the heart (with the notable exception of the pulmonary veins).
The true distinction lies in the architecture of their walls, adapted to the pressure and volume demands each system supports.
Exclusive comparative table (Artery vs. Vein)
Systematizing knowledge is the first step toward clinical mastery. Use this table as your quick reference:
| Feature | Artery (Resistance Vessels) | Vein (Capacitance Vessels) |
| Direction of Flow | Efferent (Heart → Tissues) | Afferent (Tissues → Heart) |
| Classic Gas Content | Oxygenated Blood (exception: Pulmonary Artery) | Deoxygenated Blood (exception: Pulmonary Veins) |
| Hemodynamics / Pressure | High Pressure (Pulsatile; Normal systolic < 120 mmHg) | Low Pressure (Laminar Flow; 5–15 mmHg) |
| Wall Structure | Thick, Elastic, Muscular, Non-distensible | Thin, Less elastic, Distensible |
| Tunica Media | Predominant (Abundant smooth muscle and elastin) | Thin (Lesser muscular component) |
| Lumen (Vessel Cavity) | Smaller, Circular, and Regular | Larger, Irregular, and Collapsible |
| Valves | Absent (except for valves at the origin of great vessels) | Present (Semilunar; Crucial for unidirectional flow) |
| Pulsation | Present, Palpable, and Visible | Absent |
| Location | Generally deep | Superficial and Deep |
| Macroscopic Appearance | Bright red (Saturated), Pulsating | Dark blue (Deoxygenated), Collapsible |
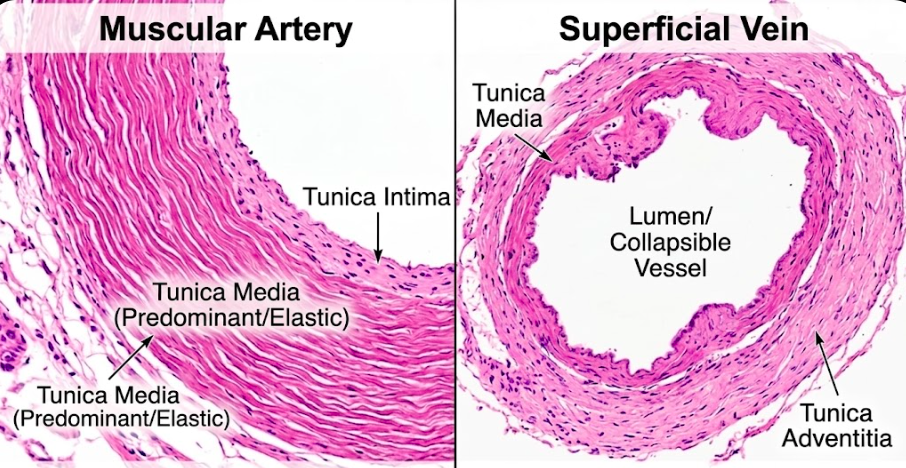
Vascular histology: the architecture of the vessel wall
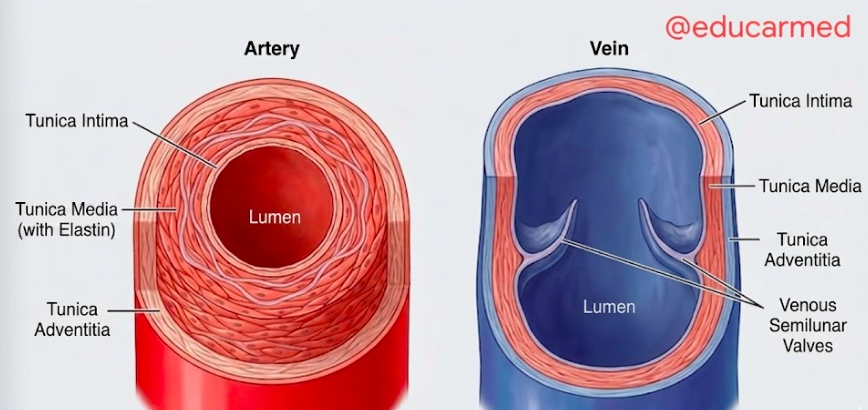
Both arteries and veins share the basic structural organization of three tunics: intima, media, and adventitia. However, the relative thickness and composition of these layers vary drastically to meet their physiological functions:
1. Elastic Arteries (Conducting Vessels) Examples: Aorta, Brachiocephalic Trunk, Common Carotid Arteries.
- Tunica Media: Extremely thick, characterized by multiple concentric lamellae of elastin. This architecture allows the vessel to expand to absorb the stroke volume and then recoil (elastic recoil), maintaining diastolic pressure and continuous flow (Windkessel Effect).
2. Muscular Arteries (Distributing Vessels) Examples: Brachial, Radial, Femoral.
- Tunica Media: Composed predominantly of smooth muscle cells. Sympathetic innervation of these cells regulates the vessel diameter (vasoconstriction and vasodilation), controlling peripheral vascular resistance and regional blood flow.
3. Veins (Capacitance Vessels)
- Tunica Media: Significantly thinner than that of corresponding caliber arteries. The tunica adventitia is often the thickest layer in large veins. The lumen is larger and irregular, reflecting low pressure.
- Venous Valves: The crucial mechanism for venous return, especially in the lower extremities, lies in the semilunar valves. Formed by folds of the tunica intima, they prevent gravity-induced blood reflux.
Physiology and hemodynamics: high pressure vs. high volume
Anatomical differences form the foundation for hemodynamic function:
- Arterial System: Operates as a high-pressure, pulsatile system designed to ensure continuous tissue perfusion. Its wall must be rigid enough to withstand systolic pressure and elastic enough to maintain diastolic pressure.
- Venous System: Operates as a low-pressure, laminar flow system, acting as the body’s main blood reservoir (capacitance vessels). Approximately 65–70% of total blood volume is found in the veins. Venous return depends not on residual pressure, but on auxiliary mechanisms:
- Skeletal Muscle Pump: Contraction of lower limb muscles compresses deep veins, propelling blood upward.
- Venous Valves: Ensure unidirectional flow.
- Respiratory Pump: Negative intrathoracic pressure during inspiration “sucks” blood toward the right atrium.
Clinical importance and vascular semiology
This is where knowledge transforms into action. The differences between artery and vein directly impact physical examination and invasive procedures:
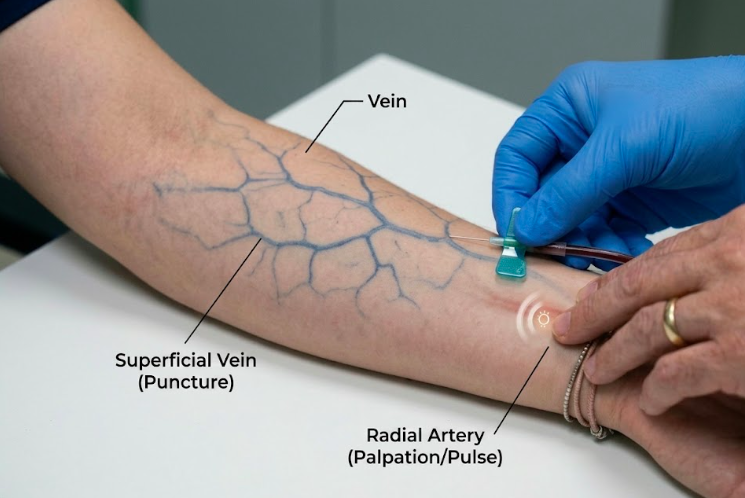
- Punctures and Access: For peripheral blood draws and volume/medication administration, we prefer the superficial venous system due to its accessibility, low pressure (lower risk of hematoma), and collapsible wall. If an accidental arterial puncture occurs, identified by bright red, pulsatile blood, vigorous manual compression for 5 to 10 minutes is mandatory.
- Catheterization and Monitoring: We reserve the arterial system (radial or femoral artery) for highly complex procedures, such as invasive arterial blood pressure monitoring (MAP) or cardiovascular interventions. For central venous access, we use the internal jugular or subclavian veins, which offer a direct path to the right atrium.
- Vascular Pathologies: Understanding the structure helps differentiate diseases. Aneurysms (dilatations) are more common in the high-pressure arterial system (aorta), while thrombosis (clot formation) and valvular insufficiency are typical pathologies of the capacitance venous system (lower limbs).
- Physical Examination: A palpable and visible arterial pulse is the direct manifestation of systolic pressure. In the venous system, engorgement of the external jugular veins is a semiological sign of right-sided heart failure or elevated central venous pressure.
FAQ – exceptions every student misses on the exam
Do not forget the exceptions that challenge classical knowledge:
- Pulmonary Artery: Carries deoxygenated blood from the right ventricle to the lungs.
- Pulmonary Veins: Carry oxygenated blood from the lungs to the left atrium.
- Umbilical Veins: Carry oxygenated blood from the placenta to the fetus.
Mastering the distinction between artery and vein is not just about memorizing comparative tables. It is about understanding how vascular architecture is designed to meet the body’s hemodynamic demands and how these differences directly impact our clinical conduct, physical examination, and patient safety.
About @EducarMed
Educar Med isn’t just about passing tests; it’s about rejecting clinical mediocrity. We are a community dedicated to training the new generation of physicians who think, examine with precision, and transform lives.
Keep raising your clinical standards. Follow us on social media: