Right upper quadrant (RUQ) abdominal pain, especially after fatty meals, is a very common presentation in the Emergency Department (ED). The most common mistake is treating all of these cases simply as “biliary colic” without identifying signs of gallbladder inflammation, common bile duct obstruction, or an associated infection.
Although these conditions share risk factors and can occur sequentially, they involve entirely different anatomical locations and levels of severity. The key is understanding where the gallstone is located and what repercussions it is causing.
This content is for educational purposes and does not replace medical evaluation, physical examination, laboratory testing, or imaging.
The biliary tract mental map
The gallbladder stores bile. When you eat a meal, especially one rich in fat, it contracts to release bile into the intestine.
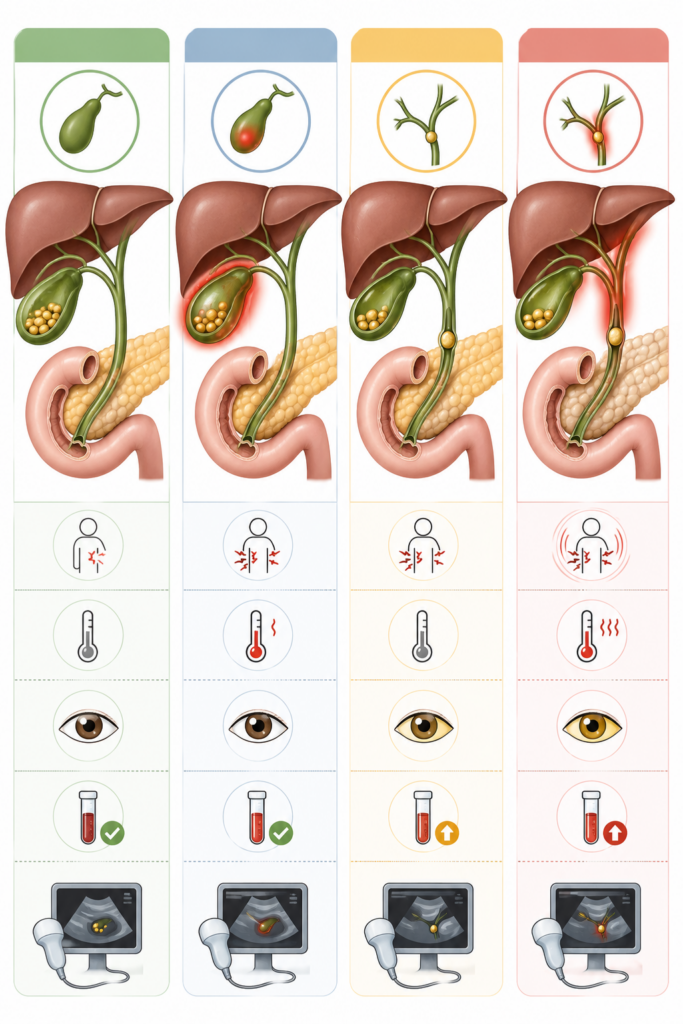
A gallstone can remain in the gallbladder, obstruct the cystic duct, or migrate into the common bile duct (CBD), the main pathway that carries bile to the duodenum. The location and duration of the obstruction determine the clinical picture:
- Transient obstruction of the cystic duct: Biliary colic.
- Persistent obstruction of the cystic duct with gallbladder inflammation: Acute cholecystitis.
- Gallstone in the common bile duct: Choledocholithiasis.
- Biliary obstruction associated with infection: Acute cholangitis.
1. Biliary colic: pain from transient obstruction
Biliary colic generally occurs when a gallstone temporarily obstructs the cystic duct. The gallbladder attempts to contract against this obstruction, causing severe pain. Despite its name, which is used historically due to the episodic and recurrent nature of the attacks the pain is usually constant, not wave-like or colicky. It appears suddenly, reaches high intensity, and generally lasts for less than six hours. It is commonly located in the right upper quadrant (RUQ) or epigastrium, often radiating to the back or right shoulder. Nausea and vomiting may also be present.
The patient usually does not have a fever, signs of systemic toxicity, jaundice, or persistent alterations in liver enzymes. Between attacks, the patient may be completely asymptomatic.
A right upper quadrant ultrasound typically shows gallstones without relevant inflammatory signs. In typical cases, initial management involves analgesia, clinical evaluation, and scheduling an elective cholecystectomy based on surgical indication.
2. Acute cholecystitis: gallbladder inflammation
Acute cholecystitis occurs when the obstruction of the cystic duct persists. Biliary stasis and gallbladder distension trigger inflammation; in some cases, there is a secondary bacterial infection. The pain is more persistent, generally lasting longer than six hours, localized in the RUQ, and associated with local tenderness. Fever, nausea, vomiting, and leukocytosis are frequent findings.
Murphy’s sign may be present: it is important to remember that this is not just pain upon deep palpation, but rather the sudden arrest of inspiration caused by pain when the examiner palpates the gallbladder fossa (RUQ) during a deep breath.
On ultrasound, findings that support the diagnosis include gallstones, gallbladder wall thickening (> 3-4 mm), pericholecystic fluid, gallbladder distension, and a positive sonographic Murphy’s sign.
Cholecystitis does not usually cause significant obstructive jaundice or dark urine. A rare exception is Mirizzi syndrome, where a large gallstone impacted in the infundibulum or cystic duct causes extrinsic compression of the common bile duct. If jaundice and dark urine appear outside this context, you must suspect a stone in the CBD (associated choledocholithiasis).
Treatment involves supportive care, analgesia, antibiotics when indicated, and surgical consultation for an early cholecystectomy, depending on the patient’s stability and overall context.
3. Choledocholithiasis: gallstone in the common bile duct
Choledocholithiasis is the presence of one or more gallstones in the common bile duct (CBD). Frequently, the stone forms in the gallbladder and migrates into the main biliary tract. This condition should be suspected when biliary pain is associated with signs of cholestasis or biliary obstruction. The most important findings include jaundice, dark urine (choluria), pale stools (acholic stools), and elevated direct bilirubin, alkaline phosphatase (ALP), and gamma-glutamyl transferase (GGT).
Dark urine occurs because conjugated bilirubin, which should be eliminated through bile, accumulates in the blood and is filtered by the kidneys. Meanwhile, ALP and GGT increase as an expression of cholestasis and damage to the biliary epithelium. Abdominal ultrasound is usually the first imaging test. It can show intra- or extrahepatic biliary dilation and, in some cases, the stone itself within the CBD. However, an ultrasound without visible stones does not rule out choledocholithiasis. When suspicion remains high, Magnetic Resonance Cholangiopancreatography (MRCP) or an Endoscopic Ultrasound (EUS) may be necessary.
ERCP (Endoscopic Retrograde Cholangiopancreatography) should not be used merely as a routine diagnostic test when less invasive alternatives exist. Its role is primarily therapeutic, allowing for the decompression of the biliary tract and stone extraction in selected patients.
Choledocholithiasis is not synonymous with cholangitis. A patient can have biliary obstruction without infection, but they must be closely monitored, as the obstruction can progress to severe complications like acute cholangitis and gallstone pancreatitis.
4. Acute cholangitis: infection over an obstructed biliary tract
Acute cholangitis is a bacterial infection of the biliary tree, usually precipitated by an obstruction. In clinical practice, CBD stones are one of the most frequent causes. The diagnosis should be considered when there is evidence of systemic inflammation associated with cholestasis or biliary obstruction. Fever, chills, leukocytosis (or leukopenia in severe cases), and elevated CRP reinforce the suspicion of infection. Jaundice, dark urine, and increased direct bilirubin, ALP, and GGT point to the obstruction.
Charcot’s triad is the classic presentation: RUQ pain, fever, and jaundice. It is highly suggestive when present, but its absence does not rule out cholangitis. Hypotension and altered mental status, added to Charcot’s triad, make up Reynolds’ pentad and indicate an extremely severe disease (biliary septic shock), with a high risk of multi-organ failure and death.
Acute cholangitis is an absolute medical emergency. Management includes aggressive fluid resuscitation and ICU support, broad-spectrum intravenous antibiotics, and urgent biliary drainage, usually performed via ERCP.
Quick comparison for the ER
| Condition | Most Likely Site of Obstruction | Pain Profile | Fever / Systemic Inflammation | Cholestasis & Jaundice | Key Imaging/Workup |
| Biliary Colic | Cystic duct, transient | Severe, constant, usually < 6 hrs | Absent | Usually absent | Ultrasound |
| Acute Cholecystitis | Cystic duct, persistent | Persistent, usually > 6 hrs (Murphy +) | Frequent | Usually absent or mild | Ultrasound |
| Choledocholithiasis | Common Bile Duct (CBD) | Biliary pain may be present | May be absent | Frequent (Elevated direct bili, ALP, GGT) | US + MRCP or EUS |
| Acute Cholangitis | Obstructed CBD + Infection | Abdominal pain (Charcot’s Triad) | Fever, chills, leukocytosis, sepsis | Frequent | Labs + Imaging (Therapeutic ERCP) |
How to reason in the emergency department
In a patient with right upper quadrant pain, the first question isn’t just “Do they have gallstones?” The most useful and life-saving question is: “Is there evidence of localized inflammation, common bile duct obstruction, or systemic infection?”
- Postprandial pain, no fever, no jaundice, and normal labs point to biliary colic.
- Persistent pain, positive Murphy’s sign, fever, leukocytosis, and sonographic signs of local inflammation point to acute cholecystitis.
- When dark urine, jaundice, elevated direct bilirubin, ALP, and GGT appear, the hypothesis of choledocholithiasis takes priority.
- If fever, chills, highly elevated inflammatory markers, or hemodynamic instability are added to this obstructive pattern, the diagnosis is acute cholangitis until proven otherwise.
Red flags not to ignore
Biliary colic, cholecystitis, choledocholithiasis, and acute cholangitis are not just different names for “having gallstones.” They represent distinct clinical stages and complications of biliary disease.
Recognizing these patterns quickly and accurately allows providers to avoid minimizing a mild obstructive episode or fatally delaying the referral of a severe biliary emergency.
To continue studying real clinical cases and improving your decision-making on shift, explore other articles on educarmed.com and follow us on social media!
About Educar Med
Educar Med isn’t just about passing tests; it’s about rejecting clinical mediocrity. We are a community dedicated to training the new generation of physicians who think, examine with precision, and transform lives.
Keep raising your clinical standards. Follow Educar Med on social media: